
Dr. Matthew Edwards and Dr. Cullen McCarthy from Wake Forest School of Medicine discuss management of Renal Vascular diseases
Script by Dr. Cullen McCarthy
Dr. Matthew Edwards is a professor and chair of Vascular and Endovascular Surgery at Wake Forest School of Medicine, he completed his General Surgery residency at North Carolina Baptist Hospital followed by a Vascular Surgery fellowship at Wake Forest.
Dr. Cullen McCarthy is a first year Vascular Surgery fellow at Wake Forest School of medicine. He attended medical school at University of South Alabama followed by a General surgery Residency at University of Oklahoma
Q: What is renovascular hypertension and ischemic nephropathy?
A: Hypertension as a result of progressive renal artery stenosis
-
While renal artery stenosis is a relatively common finding in older patients with hypertension, it’s relatively uncommon as the primary cause of hypertension.
Q: What is ischemic nephropathy?
A: Decreased renal function and/or chronic kidney disease that results from atherosclerotic renal artery stenosis due to a reduction in glomerular filtration rate (GFR) and rise in creatine produced by any cause of diminished renal blood flow that threatens
Q: Who is at risk for ischemic neuropathy?
A: Renal injury can develop in anyone with a kidney or kidney region beyond a critically stenotic artery
-
Now, this is usually in patients with atherosclerotic disease, but any flow limiting lesion—such as coarctation of the aorta, mid-aortic syndrome, or fibromuscular dyplasia-- can cause ischemic neuropathy OR renovascular hypertension.
-
In terms of clinical practice, the prevalence of renovascular hypertension is probably less than 1 % in patients with mild hypertension but may be as high as 10 to 40 % in patients with acute (even if superimposed on a preexisting elevation in blood pressure), severe, or refractory hypertension.
Q: That’s the best you can do, 10-40%? That’s a big window.
A: Yes, and it illustrates the biggest issue we have with renovascular disease. We know 5-22 % of patients 50 years or older who have advanced CKD have some degree of renal artery stenosis and 23 to 54% of these patients have bilateral renal artery disease.
-
Bilateral renal arterial stenosis is associated with more widespread atherosclerotic disease, higher serum creatinine levels, and higher mortality than unilateral disease
-
Renal artery revascularization among patients in these studies infrequently produced a meaningful recovery of kidney function, which would have supported the diagnosis
Q: So not everyone with flow limitations to their renal vascular will get renovascular hypertension or ischemic neuropathy?
A: Not at all, actually. Flow limiting lesions may be an "incidental" finding in patients who have CKD or hypertension that is caused by a separate disorder (eg, diabetic nephropathy and essential/primary hypertension).
-
Because of this, it can be very difficult to distinguish between patient whose disease is induced by renal artery stenosis and those who have alternative causes of CKD or renovascular hypertension.
Q: So you’re telling me that we have no idea who has clinically significant disease and who doesn’t?
A: No. Fortunately there are clinical findings that suggest that renovascular disease is an underlying cause:
-
Recent or rapid development of severe hypertension.
-
-
Relatively specific for renovascular hypertension and is the strongest predictor of antihypertensive benefit from revascularization.
-
-
Severe hypertension that may be treatment resistant.
-
-
Some patients with ischemic nephropathy are normotensive, which may be due in part to a reduced cardiac output
-
-
Acute rise in serum creatinine following the administration of angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs).
-
-
Rise in serum creatinine is more common with agents that block the renin-angiotensin system than with other antihypertensive drugs because glomerular filtration rate (GFR) often depends upon the efferent arteriolar actions of angiotensin II in this setting.
-
More common with bilateral as compared with unilateral disease because there is hemodynamic compromise to the entire renal functional mass
-
This usually resolves after withdrawal of the drug.
-
Restoring the renal blood supply in such cases can recover the ability to use these drugs for blood pressure control.
-
-
Significant variability of serum creatinine concentration that may be due to changes in volume status
-
A rapid rise in arterial pressure associated with sudden development of left ventricular failure ("flash pulmonary edema").
-
-
This finding is more common with renal artery stenosis because bilateral disease is also associated with diuretic resistance and sympathetic adrenergic activation
-
-
Deterioration of kidney function after placement of an endovascular aortic stent graft-- IATROGENIC
Q: So it matters which kidney is affected or if it’s one or both?
A: Yes, effect of the stenosis may not be clinically apparent due to compensatory function of the unaffected contralateral kidney
-
Most cases of renal artery stenosis affect one side much more than the other; one kidney is affected with the second kidney being essentially normal, hence the designation "unilateral" disease.
-
Patients who are diagnosed with ischemic nephropathy usually have high-grade stenosis of both renal arteries or stenosis to a solitary functioning kidney.
-
-
It is this subpopulation of the disease that merits specific consideration because of its additional contribution to fluid retention, loss of kidney function, and congestive heart failure.
-
Q: What are the pathophysiological mechanisms at play here?
A: Like we said, first you need a flow limitation. We mentioned several, but by in large There are two major causes of renal artery stenosis:
-
1) Atherosclerosis – you’ll generally see this in patients over 45 years old, likely with known PVD/CAD—though it can occur as an isolated renal lesion—usually involving the aortic orifice or the proximal main renal artery.
-
2) Fibromuscular dysplasia – These patients are most often women under the age of 50 years and typically involves the mid- or distal main renal artery or the intrarenal branches.
-
-
Rarely iatrogenic from malposition or migration of endovascular aortic stent grafts over the renal orifices.
-
Q: Okay, I think the flow limitation part has been well established. What next?
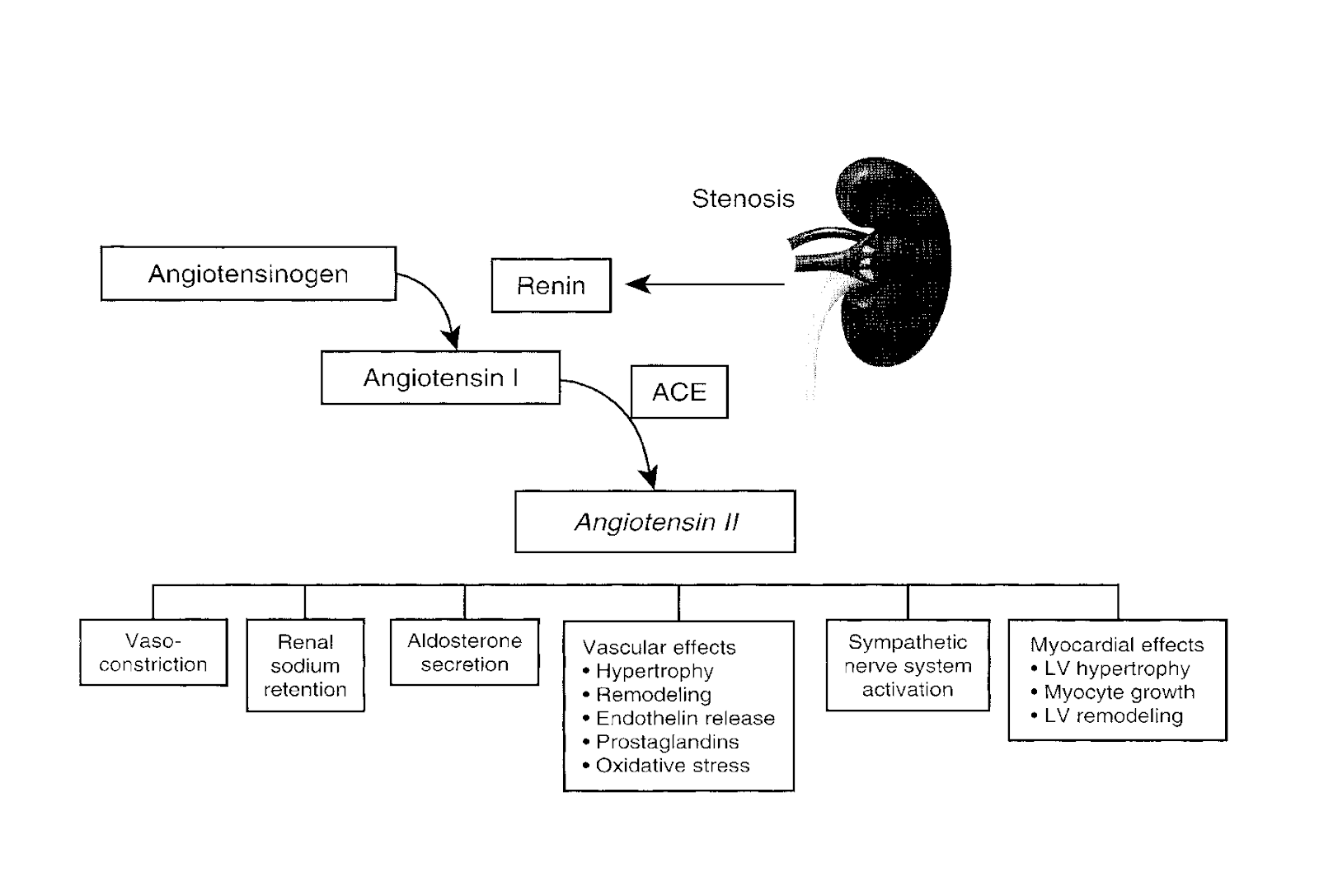
A: Renal (especially bilateral) hypoperfusion induces activation of the renin-angiotensin-aldosterone system which increases vascular tone and impairs sodium excretion resulting in expansion of the extracellular fluid volume.
Q: Ok, can’t we just treat their hypertension and give these patients an ACE inhibitor at this point?
A: Sure. And oftentimes we do. In fact, many of these patients can be treated with medical therapy without loss of function or irreversible fibrosis, sometimes for many years
-
Studies in human subjects demonstrate that, despite a moderate reduction in renal perfusion pressure (up to 40 %) and in renal blood flow (mean 30 %), glomerular filtration is reduced but tissue oxygenation within the kidney cortex and medulla can adapt without the development of severe hypoxia.
-
But this only works to an extent.
Q: Explain that…
A: As the hypertension is treated, we’re lowering the pressure gradient across the stenosis and can actually increase the degree of renal malperfusion and worsen the renal function.
-
Oftentimes this loss of kidney function is a reversible consequence of antihypertensive therapy but it to some degree limits our ability to control the hypertension medically without causing further damage to the kidneys…. And it can also reflect progressive narrowing of the renal arteries and/or progressive intrinsic kidney disease as more advanced vascular occlusion, corresponding to a 70 to 80% narrowing of the renal artery, leads to demonstrable cortical hypoxia.
Q: Can we tell who has cortical hypoxia through diagnostic tests?
A: To some degree. Cortical perfusion can be measured by blood oxygen level dependent magnetic resonance (BOLD-MR). Additionally, inflammatory markers sampled from renal veins of stenotic kidneys correlated strongly with the degree of hypoxia (as measured by BOLD-MR), particularly after correction of the stenosis with angioplasty
Q: Ok, so we have a patient with evidence of malperfused kidneys, either through worsening renal function or uncontrolled hypertension, with known discrete stenoses, and we even got a BOLD-MRI which confirms it. Let’s just revascularize them and be done with it?
A: Not so fast. Although vascular stenosis or occlusion can initiate these processes, long-standing ischemia causes parenchymal injury characterized by inflammation and fibrosis which eventually becomes an irreversible process. At some point, restoring renal blood flow provides no recovery of kidney function or clinical benefit.
Q: So how can we determine who has CKD or hypertension due to renovascular stenosis that we can actually help?
A: This is probably the most important question since in this whole disease process.
-
To start, if a patient has the clinical manifestations of ischemic nephropathy or renovascular hypertension as we discussed above, a presumptive diagnosis of ischemic nephropathy can be made if there is radiologic documentation of significant stenosis (usually more than 70 % luminal occlusion) of both renal arteries or of one renal artery to a solitary functioning kidney.
Q: But how do we know the vascular occlusive disease posing critical hemodynamic limitation to kidney function?
-
Generally, luminal occlusion of at least 60 to 75 % is required to limit blood flow and reduce perfusion pressure
-
This degree of stenosis is usually associated with a measurable translesional “pull-back” pressure gradient of 10 to 15 mmHg.
-
Doppler ultrasound criteria conventionally require peak systolic velocities above 180 to 200 cm/sec to identify more than 60 % luminal stenoses but identifiable levels of cortical hypoxia (measured by blood oxygen level dependent magnetic resonance [BOLD-MR]) are usually associated with translesional velocities above 385 cm/sec or reduction of single kidney glomerular filtration rate (GFR) in the range of 20 to 25 mL/min.
Q: Most importantly: is the condition of the kidneys such that restoring renal blood flow is likely to benefit function?
Short answer, we still can’t be certain.
-
Long answer, we can at least have some idea by considering the renal resistive index, the six-month trajectory of kidney function, and the size of the kidneys
-
-
or by performing a kidney biopsy (which is not usually done).
-
-
None of these factors predict the outcome of revascularization with certainty.
-
-
Improved and validated methods to evaluate the salvageability of kidney function in this disorder are greatly needed and are the holy grail of this disease process.
-
Q: Ok, let’s go through some of these: Renal Resistive index:
A: Some studies indicate that elevated resistive indices in segmental vessels (above 0.80) measured by duplex ultrasound denote poor prognosis for renal recovery while a low resistive index is a favorable sign.
Trajectory of kidney function
The most consistent predictor of good recovery of kidney function after revascularization has been a recent deterioration of kidney function (ie, in the prior six to twelve months).
Kidney size
Very small kidneys (less than 7 cm in longest diameter) are usually considered unlikely to recover after revascularization.
Kidney biopsy
Previous studies suggest that biopsy demonstrating preexisting atheroembolic changes and interstitial fibrosis indicate a limited potential for recovery.
-
Biopsies are not usually performed.
Comparison of kidney morphology with kidney function
Some investigators have recommended assessing morphologic parameters, such as renal parenchymal volume and cortical thickness with MRI, and comparing these parameters with kidney function measured by radionuclide scanning
-
In a stenotic kidney, apparently normal morphology combined with reduced function may indicate a "hibernating kidney" that could be salvaged with revascularization.
Q: So how do we get a definitive diagnosis?
A: A definitive diagnosis is not usually made before revascularization. In practice, confirmation of the diagnosis is based upon stabilization or improvement of the GFR after successful revascularization.
Q: Ok, at least now we think our patient’s renal artery stenosis maybe is causing hypertension or decline in renal function and we can possibly reverse it… how do we treat it?
A: For starters, all of these patients should receive medical therapy to control their hypertension in addition to routine CKD care and surveillance. They need to be aggressively treated for secondary prevention of cardiovascular morbidity with aspirin, statins, cessation of smoking, and, in patients with diabetes, glycemic control.
Second, once diagnosis has been made we have 2 therapeutic alternatives…
Which are?
A: First, medical therapy alone- this generally involves ACE-I or ARB and as we discussed.
Hemodynamically mediated acute kidney injury is the major limitation of ACE inhibitors and ARBs in patients with bilateral renal artery stenosis as lowering the systemic blood pressure is more likely to reduce the renal perfusion and thus the intraglomerular pressure below the limits of renal autoregulation… in turn lowering the GFR.
Q: Okay, in other words we can have chronic normalization of the systemic pressure that might eventually lead to ischemic atrophy due to the reduced renal perfusion pressure distal to the stenosis? Any other concerns with medical management alone?
A: We’re addressing or prevention progression of stenosis in those with atherosclerotic disease.
Q: Ok, since this isn’t a vascular medicine podcast, what’s our other option?
A: Procedural intervention (open or endovascular) along with medical therapy.
Now you’re talking. Who should we fix operatively?
-
A: Some but not all patients should undergo revascularization, Patient selection single most important factor.
-
-
Depends upon the hemodynamic severity and likely recoverability of kidney function
-
Q: You mentioned recoverability before, can you once again touch on what helps us determine recoverability?
-
Recoverability indicators--
-
-
A short duration of blood pressure elevation prior to the diagnosis of renovascular disease, since this is the strongest clinical predictor of a fall in blood pressure after renal revascularization
-
Failure of optimal medical therapy to control the blood pressure
-
Intolerance to optimal medical therapy (eg, deterioration of renal function during antihypertensive drug therapy)
-
Recurrent flash pulmonary edema and/or refractory heart failure
-
Otherwise unexplained progressive renal insufficiency, particularly if proteinuria is absent
-
Q: But do we have any good data proving our interventions help?
A: This is where things can get muddy.
Early on, observational studies demonstrated a high rate of procedural success with percutaneous transluminal renal angioplasty (PTRA) and stent placement (~85%) in patients with ostial atherosclerotic disease, as well as a high rate of clinical success measured by improvements in blood pressure and kidney function in 50 to 75 % of subjects.
Q: Anything better than observational studies?
A: Unfortunately, randomized trials showed no additional benefit from stenting when added to medical therapy with respect to blood pressure control, renal function, cardiovascular events, and mortality. But these studies have their own limitations.
The one we keep hearing about is the CORAL trial. Tell me about that.
-
CORAL trial
-
-
Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) trial
-
947 patients (80 % had unilateral disease) who met the following two criteria:
-
-
Unilateral or bilateral atherosclerotic renal artery stenosis >60 % if diagnosed with conventional angiography, peak systolic velocity >300 cm/second if diagnosed by duplex Doppler ultrasonography, Luminal narrowing >80 % if diagnosed with magnetic resonance angiography or computerized tomography angiography (or >70 % with additional evidence of renal ischemia)
-
Systolic hypertension despite two or more antihypertensive medications and/or an estimated glomerular filtration rate (eGFR) <60 mL/min/1.73 m2 that was presumably due to the stenosis.
-
All patients received antiplatelet therapy plus best medical therapy including ARB
-
-
Revascularization had no additional effect on the primary outcome (a composite of cardiovascular or renal death, stroke, myocardial infarction, hospitalization for heart failure, a reduction in eGFR by more than 30 %, or end-stage renal disease) as compared with medical therapy alone (35.1 versus 35.8 %).
-
No effect on any of the individual components of the primary outcome.
-
Low procedural complication rate ~2%
-
Well, that sounds pretty convincing.
-
Limitations on existing treatment data:
-
-
Considerable selection bias – For the most part, the patients enrolled in these trials did not meet the criteria for selecting patients likely to benefit from intervention (eg, short duration of blood pressure elevation, hypertension resistant to medical therapy, recurrent flash pulmonary edema):
-
-
CORAL
-
-
Patients hospitalized for heart failure within 30 days of screening for the trial were excluded, thereby limiting the number of trial participants with recurrent flash pulmonary edema.
-
Mean number of antihypertensive medications used by CORAL participants at baseline was 2.1- many had not failed optimal medical therapy
-
More than 25 % had controlled blood pressure upon entry into the trial.
-
Mortality and event rates lower than in most previous registries, suggesting that many high-risk patients were not enrolled.
-
-
ASTRAL
-
-
Large number of patients had stenoses that were probably not clinically significant (50 to 70 %), and patients were excluded if their primary doctors felt that they "definitely" needed revascularization.
-
-
-
Results of the trials differ substantially from observational reports of "high-risk" subsets
-
-
For the most part, patients selected by their treating clinicians to undergo revascularization have derived greater benefit from revascularization than did patients enrolled in the trials who were randomly assigned to revascularization
-
-
Ok, we’ve determined our patient is an appropriate candidate for intervention, and we don’t fully buy into CORAL, what can we do?
-
Percutaneous renal angioplasty/stenting in addition to medical therapy
-
-
Most commonly employed if technically feasible.
-
Most amenable lesions to angioplasty are those producing incomplete occlusion in the main renal artery.
-
-
Total occlusions and ostial lesions extending into aorta generally do not respond well to angioplasty alone due to elastic recoil.
-
-
Quick results: maximum antihypertensive response is generally observed at 48 hours after the procedure
-
-
But BP levels and antihypertensive drug requirements often change over subsequent weeks
-
-
In general, the effects of revascularization on blood pressure were greater in bilateral disease, but effects on renal function and mortality did not differ in those with bilateral as compared with unilateral stenosis .
-
Most atherosclerotic lesions are now treated with primary stenting to avoid rapid development of restenosis.
-
-
A higher initial primary success rate, defined as less than 50 % stenosis (88 versus 57 %).
-
At six months, a higher patency rate (75 versus 29 %) and a lower restenosis rate (14 versus 48 %).
-
Twelve patients assigned to PTRA alone underwent stenting because of treatment failure within six months. These patients had a similar blood pressure response as those initially treated with stenting.
-
-
What about complications?
-
Complication rate with percutaneous transluminal renal angioplasty with or without stenting is between 5 and 15 %
-
-
Mostly minor: puncture site hematoma and renal artery dissection.
-
Serious complications more rare: renal artery thrombosis or perforation, AKI 2/2 atheroembolic disease (~1%)or radiocontrast agent injury.
-
Mortality exceedingly rare
-
Outcomes data
-
In the correct patient population:
-
-
Unilateral disease
-
-
PTRA alone results in normalization of blood pressure (removal of antihypertensive drug therapy) ~8-20%
-
Some improvement 50-60%
-
Failure rate ~20-30%
-
Restenosis rate of 8 to 30 % at two years (without stent)
-
Better results with unilateral fibromuscular disease.
-
Less consistent for patients with chronic hypertension compared with patients who have an acute elevation in blood pressure
-
-
Bilateral disease
-
-
25-30% will recover kidney function to a meaningful degree, sometimes avoiding progression to end-stage kidney disease (ESKD) and/or the need for renal replacement therapy.
-
~50% will have little immediate change in kidney function but will "stabilize"
-
~20% will have a progressive deterioration of kidney function, sometimes related to the procedure
-
-
Guidelines
-
2006 ACC/AHA guidelines on peripheral artery disease recommends that a stent be placed in patients undergoing PTRA for treatment of atherosclerotic renal artery stenosis
-
-
PTRA without stent placement is rarely performed unless the anatomy precludes stenting.
-
POBA without stenting is generally less successful and associated with more complications (eg atheroemboli)
-
How durable is PTA/stenting?
-
Restenosis
-
-
~11-17%
-
-
11-39% during the first one to two years
-
-
Detected as a rise in blood pressure requiring more intensive therapy
-
Angioplasty/stenting injures the vascular endothelium, which may result in restenosis.
-
Symptomatic stenosis leading to a rise in blood pressure or a fall in GFR are less common and are reported in 10 to 20 % of patients
-
How do you follow these patients after stenting?
-
Follow-up of patients who have had a renal artery stent should include serial measurements of blood pressure and estimation of GFR.
-
-
Post-stent duplex ultrasound @2-4weeks with
-
Repeated examinations on a quarterly basis (not much data)
-
Patients who develop an increase in pressure or reduced GFR after stenting should undergo duplex ultrasonography to identify restenosis
-
Retreatment with angioplasty with or without repeat stenting can be attempted, but the restenosis rate after repeat angioplasty is increased.
-
-
Surgical reconstruction may be pursued in patients with recurrent episodes of restenosis and loss of kidney function.
-
-
What about an open operation?
-
Surgical revascularization used in addition to medical therapy
-
-
Less common since the widespread application of effective antihypertensive drug therapy and endovascular stents (mid 90s)
-
So who still gets open repair?
-
Primarily for correction of complex vascular lesions and/or repeated episodes of in-stent restenosis
How do we do it?
-
Involves bypassing the stenotic segment or of removing a small atrophic kidney with nearly complete arterial occlusion.
-
-
From the aorta or hepatorenal or splenorenal bypass to avoid diseased aorta.
-
Bilateral: either bilateral repair or unilateral repair with contralateral nephrectomy of a nonfunctioning, atrophic kidney.
-
How do outcomes compare to PTA/stenting?
-
Equally or more effective than PTRA in the treatment of atherosclerotic disease, with cure of or improvement in the hypertension occurring in 80 to 95 % of patients.
-
-
Cure of hypertension after surgery is most likely in patients who have been hypertensive for less than five years
-
-
Lack of complete response was usually associated with one of two factors:
-
-
Presence of underlying primary/essential hypertension
-
Development of intrarenal vascular disease due to exposure of the contralateral kidney to the elevated blood pressure.
-
Guidelines recommendations?
-
2005 American College of Cardiology/American Heart Association (ACC/AHA) guidelines:
-
-
Open surgery in patients with atherosclerotic renal artery stenosis largely restricted to those who have multiple small renal arteries, have early primary branching of the main renal artery, require aortic reconstruction near the renal arteries for other indications (eg, aneurysm repair or severe aortoiliac occlusive disease), or to avoid manipulation of a highly diseased aorta or failed endovascular stents (using specific surgical techniques, including splenorenal, ileorenal, or hepatorenal bypass procedures).
-
So why not do it instead of stent?
-
In-hospital mortality: ~3-10 % in high volume centers
-
-
Risk factors diffuse atherosclerosis, advanced age, chronic kidney disease, heart failure, or chronic lung disease.
-
No deaths in 105 procedures for fibromuscular dysplasia (FMD).
-
You mentioned FMD as a cause of renovascular hypertension, tell me more about that…
Fibromuscular dysplasia (FMD) is a noninflammatory, nonatherosclerotic disorder that leads to arterial stenosis, occlusion, aneurysm, dissection, and arterial tortuosity.
-
Virtually always diagnosed radiographically – formerly pathologically, but rarely sent for specimen in modern diagnosis or treatment
How do we classify it?
-
Most commonly classified by angiographic appearance:
-
-
Multifocal FMD (more common)
-
-
angiographic appearance of a "string of beads."
-
corresponds pathologically to medial fibroplasia, the most common histologic type, and to perimedial fibroplasia, which is less common.
-
-
Focal FMD (less common)
-
-
angiographic appearance of a "circumferential or tubular stenosis"
-
corresponds pathologically to intimal fibroplasia but medial hyperplasia and periarterial hyperplasia may also have a focal appearance.
-
-
These two different angiographic subtypes of FMD (multifocal and focal) have different phenotypic presentations and natural history
-
-
Is FMD is, in fact, a single disease?
-
-
Where does it occur?
-
Has been observed in nearly every arterial bed
-
Involvement of the renal arteries ~75-80%
-
Involvement of the extracranial cerebrovascular arteries (eg, carotid and vertebral arteries) ~75%
-
-
2/3 of patients have multiple arteries involved.
-
Who has FMD?
-
~90% of cases in adults are in women.
-
-
No female predominance among children with FMD.
-
-
Mean age at diagnosis was 52 years, with a range of 5 to 86 years
-
-
In the past, it was believed that FMD was a disease of young women. However, older now know to make up a large proportion of affected
-
-
35-50% of cases in children and 5-10% of cases in adults under the age of 60 years with renovascular hypertension
-
Often an incidental finding:
-
-
4.4% of potential kidney donors had evidence of FMD.
-
CORAL trial:
-
-
FMD was discovered in 5.7% of the total study population (8.8% of enrolled females)
-
-
What causes FMD?
-
The etiology of FMD remains unknown
Any ideas?
-
There is some that genetics play an important role in development
-
-
Some studies report autosomal mode of inheritance with variable penetrance
-
Potential association with a single nucleotide variant in the phosphatase and actin regulator 1 gene (PHACTR1)
-
Variant rs9349379 is also a risk locus for coronary artery disease, migraine headache, and cervical artery dissection.
-
-
Predominance of young/childbearing age women hormonal influences are thought to play a role
-
-
Remains unproven.
-
-
Mechanical factors such as stretch and trauma unproven.
Does FMD present differently that the atherosclerotic renovascular disease we talked about?
-
Varies widely depending on artery affected and as it results from:
-
Ischemia related to stenosis
-
Dissection and occlusion of major arteries (renal infarction, stroke, myocardial infarction)
-
Rupture of aneurysms
-
Embolization of intravascular thrombi from dissection or aneurysms
What are the common presenting symptoms and signs
-
Manifestations of renal FMD (eg, hypertension, flank pain) are more likely to occur in men, as are arterial dissections and aneurysms.
-
-
Most common presenting signs:
-
Hypertension – 67% (66% of women and 74 % of men)
-
-
But overall hypertension is the most common manifestation of renal artery FMD in both genders
-
-
Flank pain and abdominal pain can result from ischemia, aneurysm rupture, or dissection of renal and mesenteric arteries, respectively.
-
Are these dissections common?
-
High prevalence of aneurysm and/or dissection
-
-
Aneurysm (22%) and dissection (26%).
-
-
34% of aneurysms were renal
-
11% of dissections were renal
-
-
42% had an aneurysm and/or dissection.
-
So should we screen for these dissections in a patient with known FMD?
-
Every patient diagnosed with FMD should have one-time, head-to-pelvic CTA (or MRA) is an alternative.
-
-
CTA of the neck and head on one day followed one week later by CTA of the chest, abdomen, and pelvis
-
When should we suspect FMD?:
-
Hypertension (particularly in a woman under the age of 60 years) with findings that would prompt an evaluation for secondary hypertension:
-
-
Severe or resistant hypertension.
-
Onset of hypertension before the age of 35 years.
-
A sudden rise in blood pressure over a previously stable baseline.
-
A significant increase in the serum creatinine concentration after the institution of therapy with an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) in the absence of an excessive reduction in blood pressure.
-
An epigastric/abdominal bruit.
-
-
Renal artery dissection (or carotid, vertebral, coronary)
-
Aneurysm in a visceral, carotid, vertebral, or intracranial vessel.
-
Renal infarction.
How do we diagnose this and/or distinguish it from renovascular atherosclerotic disease?
-
Confirmed by diagnostic imaging that reveals consistent findings
-
Noninvasive imaging test is usually performed first. This includes CTA, MRA, and Duplex ultrasound.
Let talk about CTA…
-
CTA is preferable due to higher spatial resolution than MRA, less dependence upon technical expertise, and a shorter scan time
-
Excellent diagnostic accuracy for FMD of the main renal arteries, although the sensitivity decreases when FMD is only present in the smaller branch renal arteries.
-
Multirow detector CT scanners, which offer more rapid image acquisition, variable section thickness, three-dimensional rendering, diminished helical artifacts, and smaller contrast requirements, may gain an increased role in the diagnosis and follow-up of renal artery FMD
What about MRA?
-
Inconsistent detection of FMD and is performed if CTA is contraindicated
-
The spatial resolution in the branch vessels is not adequate, and artifact may occur, suggesting "beading" when none is present.
-
May miss mild FMD.
-
Can be useful for detecting aneurysms and dissections
And finally, Duplex ultrasonography
-
Detects elevated blood flow velocities in the mid and distal portions of the renal artery, most common locations for FMD.
-
Increased peak systolic velocity, turbulent blood flow, and tortuosity of the mid and distal artery.
-
-
% diameter stenosis reports less helpful and usually inaccurate
-
-
lowest spatial resolution of all of the cross-sectional imaging modalities
-
most operator dependence
-
first choice only in high-volume centers with extensive expertise in this technique
What about non invasive testing?
-
DSA is performed in patients if there is a high clinical suspicion of FMD, and treatment with revascularization is planned if a stenosis is found.
-
-
Can improve visualization of the arteries by eliminating background soft tissue and bone and has higher spatial resolution than any of the other imaging modalities
-
Can measure the pressure gradient across the stenosis
-
-
Pressure decrease threshold of 10 % or more of the mean pressure should be used to decide whether a lesion is hemodynamically significant
-
IVUS and optical coherence tomography (OCT) can be helpful in determining if a dissection or intramural hematoma is present as well as help to determine if angioplasty has improved the stenosis.
-
-
Negative DSA excludes a diagnosis of FMD in the vascular bed that was imaged.
-
Any place for pathologic diagnosis in modern therapy?
-
Histopathology (and histologic classification) is no longer part of the diagnosis.
-
-
Only in the rare patient who requires surgical revascularization or resection of an aneurysm.
-
So how do we treat this, what warrants intervention and are those interventions different than what we offer atherosclerotic disease of the renal arteries?
-
All patients with FMD should be placed on antiplatelet therapy (ASA) unless otherwise contraindicated
-
Antihypertensive therapy
-
-
Most patients will require antihypertensive therapy, even if they undergo revascularization.
-
Majority of patients with focal FMD have their blood pressure cured with angoplasty
-
But what about revascularization?
-
Revascularization Goal: control of hypertension
-
-
BP can be controlled in most adults with multifocal FMD with a mean of two antihypertensive medications
-
Weigh risks and benefits in well controlled hypertension.
-
-
No randomized trials comparing revascularization with medical therapy
Well then who do we treat?
-
Recent-onset hypertension, with goal to cure hypertension.
-
Resistant hypertension despite compliance with an appropriate three-drug regimen.
-
Patients unable to tolerate antihypertensive medications or who are noncompliant with their medication regimen.
-
Adults with bilateral renal FMD, or unilateral renal FMD to a single functioning kidney, and unexplained progressive renal insufficiency thought to result from renal artery stenosis
-
Hypertensive children.
-
may be at higher risk than adults for progressive renal parenchymal loss, and therefore could benefit from revascularization even if their hypertension can be well-controlled with one or two antihypertensive medications.
And what kind of results do we get with revascularization?
-
Hypertension is cured or improved following revascularization in a large proportion of patients with FMD.
-
-
Much better than 2/2 atherosclerosis
-
Varies considerably from study to study, although hypertension control improves in most patients and depends in large part upon the definition of cure.
-
Not good data on stabilization of either GFR or renal size in patients with FMD.
-
What options do we have in terms of revascularization?
Angioplasty and open surgery
Do we have good results treating FMD with these?
-
Improvement in blood pressure (including those with and without cure) was similar with PTA as compared with surgery (86 versus 88 %).
-
Older age and longer duration of hypertension prior to revascularization were significantly associated with a lower cure rate.
How do these compare?
-
PTA achieves similar technical success and is associated with a lower risk of adverse events in observational studies
-
Most patients with FMD who are selected for renal revascularization have PTA rather than surgery
-
Major adverse events were more frequent with surgery (15 versus 6 %).
So why choose open surgery?
-
Cure rates were higher with surgery (54 versus 36 %).
-
Surgery rather than PTA if PTA fails or if the arterial anatomy is not amenable to PTA
-
-
Patients with small renal arteries (<4 mm), with branch renal artery disease, or with extensive intimal fibroplasia.
-
So how do we perform Percutaneous transluminal angioplasty for FMD?
-
Without stent placement… unlike PTA for atherosclerotic RAS
Why not place a stent?
-
Patients do very well with angioplasty alone, no reason to place a stent.
-
-
Lesion is so fibrotic that the pressure gradient cannot be obliterated with an angioplasty, a stent will not correct this problem
-
-
Such patients should be referred for surgery.
-
-
-
Usually have stenoses in the mid and distal portions of the artery rather than at the ostium or proximal portion (as occurs with atherosclerosis).
-
-
Should surgical revascularization become necessary due, for example, to in-stent restenosis, patients may require more complex branch repair to bypass the occluded stent since the stent often covers the renal artery up to the point of the first intrarenal branch.
-
Do we ever place stents?
-
Stents placed when a dissection results from the performance of PTA or in the rare instance in which a perforation of the renal artery occurs during angioplasty.
And we’re getting good outcomes with PTA alone?
-
Technical (angiographic) success rates for PTA 83-100
-
Rate of restenosis 12-34% over follow-up intervals of six months to two years
-
-
Difficult to determine if patients with FMD develop restenosis, or if the lesion was not completely treated correctly the first time.
-
Not necessarily associated with recurrent hypertension.
-
But generally we can achieve significant and sustained reductions in systolic blood pressure, diastolic blood pressure, serum creatinine, and number of antihypertensive agents.
-
Systolic blood pressure response was better in patients with FMD affecting the main renal artery than in patients with branch vessel involvement.
Any specific technical tips?
-
Cutting balloon angioplasty should be avoided
-
-
Increased risk of rupture
-
-
Post angioplasty visual inspection alone is not accurate.
-
-
Measure pressure differential using a pressure guidewire, with a mean gradient of <5 mmHg across the treated segment suggesting a satisfactory result
-
-
Measure before and after angioplasty
-
-
Post-procedure renal duplex scanning
-
-
Degree of turbulence is less prominent, and velocity elevation in the mid-distal renal artery returns to normal.
-
-
Intravascular ultrasound or optical coherence tomography (OCT) is occasionally used to evaluate the elimination or reduction of various endoluminal defects.
-
What should we do if it doesn’t work?
-
If either has no improvement in blood pressure or an initial improvement followed by recurrence, repeat angiogram and PTA.
-
-
Restenosis may actually represent inadequate angioplasty during the first procedure
-
-
Persistent HTN despite technically successful PTA suggests that the cause of hypertension is unrelated to fibromuscular disease or is related to small vessel disease within the kidney (nephrosclerosis) due to longstanding hypertension.
What kind of complications do we see after this?
-
Mostly related to vascular access
-
Rarely: renal artery perforation, dissection, or segmental renal infarction may occur.
-
Decreasing over time- 16 % in 1998 to 3 % in 2001 [39].
Ok, lets switch gears to open revascularization?
-
Aortorenal bypass with a saphenous vein graft is the most common technique
-
-
Artificial graft material used occasionally
-
For everyone? What about for pediatric patients?
-
Pediatric patients: hypogastric artery grafts are used or else aortic reimplantation of the renal artery is performed because vein grafts become aneurysmal
How does this compare again to PTA?
-
Similar success rates compared to PTA (82-89% patency) but with higher morbidity.
-
-
Perioperative mortality appears to be very low (~1.2%)
-
Usually limited to complex cases so success and complication would probably be higher if simpler cases were included.
-
What’s Monitoring and follow-up look like for these patients?
-
Medical management only:
-
-
Renal artery stenosis and kidney dysfunction may progress despite good blood pressure control
-
-
Mostly in patients with focal FMD and intimal fibroplasia
-
-
Every patient with FMD should have measurement of serum creatinine and renal artery duplex ultrasound every 12 months.
-
And After revascularization?
-
Duplex ultrasonography and serum creatinine measurements performed on the first office visit post procedure, then every six months for two years, and then yearly, if stable.
-
With worsening on new hypertension, or unexplained increase in the serum creatinine, he or she should be imaged at that time with duplex ultrasound (or CTA if the ultrasound is equivocal or poor quality).
Ok, that’s a pretty good review, but let’s switch gears and talk about renal artery aneusyms
-
Renal artery aneurysms are rare.
-
-
Autopsy studies have revealed an incidence of 0.01% to 0.09%.
-
Renal artery aneurysms are bilateral in about 10% of cases with more than 90% of true renal artery aneurysms being extraparenchymal.
-
-
Females > males
-
-
Females and males equal with FMD excluded
-
-
Most frequent site of involvement is primary bifurcation, intraparenchymal (<10%)
-
Most are saccular
-
Right slightly more common than left, bilateral 10%
-
Size criteria currently controversial*
-
-
2.5 common criteria for visceral arterial intervention, but paucity of data suggesting rupture risk drastically increases at this size
-
Many aneurysms with circumferential calcification which could offer protection against rupture
-
-
The majority of renal artery aneurysms are asymptomatic, and less than 3% rupture.
-
-
Present with flank pain, hypotension
-
10% mortality
-
90% risk of kidney loss
-
-
Although arteriosclerotic changes have been identified in most aneurysms in patients with multiple lesions, this is not a uniform finding, suggesting that arteriosclerosis may not be the most important factor in the genesis of renal artery aneurysms.
-
More likely due to a congenital medial degenerative process with weakness of the elastic lamina.
-
Fibromuscular dysplasia (FMD) is often a direct contributor to the development of an aneurysm.
-
-
Medial fibroplasia is typically associated with multiple stenoses and post-stenotic dilatation of the distal two thirds of the renal artery.
-
Renal artery aneurysms in association with FMD are generally only a few millimeters in diameter.
-
The typical angiographic appearance of a renal artery involved with medial fibroplasia is a “string of beads.”
-
-
The majority of renal artery aneurysms are saccular.
-
A rare cause of renal artery aneurysms is Ehlers-Danlos' syndrome.
-
-
This disorder is associated with extreme arterial fragility and spontaneous rupture.
-
-
Renal artery dissection caused by guide wires or catheters can occur, but is rare.
-
In an elderly patient, observation of this aneurysm with Duplex surveillance is the appropriate treatment.
-
For larger aneurysms in younger patients, aneurysmorrhaphy with primary repair or patching can be performed with low mortality.
-
-
Endovascular techniques such as coiling have been reported to be successful in treating these saccular aneurysms; however, covered stent placement may be difficult in the distal renal artery near potential branch points of the artery.
-